Get Care
Achalasia Cardia
What is Achalasia Cardia?
Achalasia cardia is a rare but serious condition that affects the esophagus, the tube that connects the throat to the stomach. In this disorder, the lower esophageal sphincter (LES)—the muscle at the bottom of the esophagus—fails to relax properly, preventing food and liquids from passing smoothly into the stomach. This dysfunction can lead to difficulty swallowing, regurgitation of food, chest pain, and other digestive issues. Over time, the condition can cause a buildup of food and liquids in the esophagus, leading to further complications.
What are the Causes Achalasia Cardia?
The exact cause of achalasia cardia is not fully understood, but it is believed to involve damage to the nerves that control the muscles of the esophagus. This nerve damage leads to the loss of coordinated muscle contractions, making it difficult for food to move into the stomach. Some potential factors include:
(1) Immune System Dysfunction (Autoimmune Response)
Achalasia is often thought to result from an abnormal response of the immune system. In this case, the body mistakenly attacks its own nerve cells—specifically, the nerve cells (called ganglion cells) located in the myenteric plexus of the esophagus. These nerves are responsible for coordinating the muscular contractions (peristalsis) that push food down the esophagus and for controlling the lower esophageal sphincter (LES), which opens to let food enter the stomach. Damage or loss of these nerves causes the muscles to lose coordination and prevents the LES from relaxing properly, which leads to the symptoms of achalasia. This immune attack may be triggered by environmental factors or infections, but in many cases, the exact reason is unclear.
(2) Genetic Factors
Although achalasia is typically considered a sporadic condition, in rare cases, it appears to run in families. This suggests that genetic mutations or inherited traits may contribute to the development of the disease in certain individuals. Some genetic syndromes, such as Allgrove syndrome (Triple A syndrome)—which includes achalasia, alacrima (lack of tears), and adrenal insufficiency—have been linked to specific gene defects. These findings indicate that for a small subset of patients, there may be a hereditary or congenital basis for the condition.
(3) Viral Infection
There is evidence suggesting that certain viral infections may be involved in the onset of achalasia. Some viruses, such as herpes simplex virus (HSV), varicella-zoster virus (VZV), or measles virus, have been found in the esophageal tissues of patients with achalasia. These infections may trigger inflammation or an immune response that damages the nerve cells in the esophagus. While the exact role of viruses is still under investigation, it’s believed that a past viral infection could contribute to or initiate the autoimmune process that ultimately leads to nerve damage.
What are the Symptoms of Achalasia Cardia?
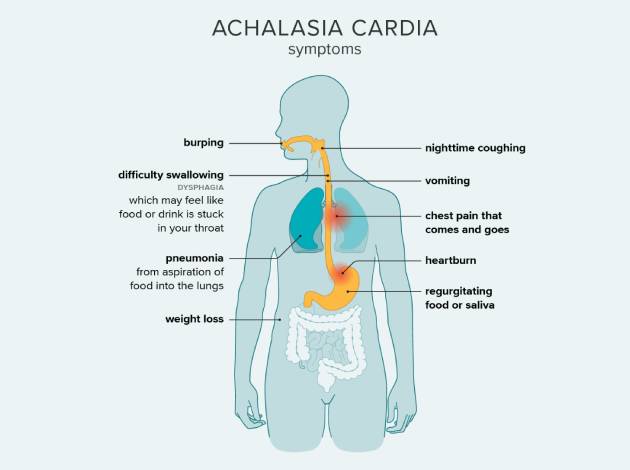
The symptoms of achalasia cardia are primarily related to difficulty swallowing and the backup of food and liquid in the esophagus. These symptoms can vary in severity and may worsen over time. Common symptoms include:
- Dysphagia (Difficulty Swallowing): One of the most prominent symptoms, making it difficult to swallow food or liquids. Solid foods are usually more difficult to swallow than liquids.
- Regurgitation: Undigested food may come back up into the throat or mouth, especially when lying down or after eating large meals.
- Chest Pain: Some patients experience chest pain that may mimic heart-related pain. The discomfort is often described as a tight or pressure-like sensation.
- Heartburn: Some people with achalasia may experience acid reflux or heartburn due to the inability of food to pass into the stomach.
- Weight Loss: Difficulty eating and swallowing can result in unintended weight loss.
- Coughing and Choking: This occurs due to food or liquids being trapped in the esophagus, leading to coughing or choking while eating or drinking.
- Bloating: A feeling of fullness or bloating, especially after meals.
What are the Risk Factors for Achalasia Cardia?
Achalasia can affect individuals of any age, though it is most commonly diagnosed in people between the ages of 25 and 60. While the precise cause remains unknown, several factors may increase the likelihood of developing achalasia:
- Age: The condition is most commonly diagnosed in adults between 25 and 60 years of age.
- Genetics: A family history of achalasia may increase the risk, suggesting a genetic predisposition.
- Gender: Achalasia can affect both men and women, though some studies suggest a slight male predominance.
- Autoimmune Disease: Some people with autoimmune conditions may be at a higher risk for developing achalasia.
What are the Complications of Achalasia Cardia?
If left untreated, achalasia can lead to serious complications, some of which may require surgical intervention. Complications of achalasia include:
- Esophageal Dilation: The esophagus may become dilated (stretched) over time due to the accumulation of food and liquids. This can worsen symptoms and cause significant discomfort.
- Malnutrition: Difficulty swallowing and regurgitation can lead to malnutrition and weight loss, as the body is unable to properly digest and absorb food.
- Aspiration Pneumonia: The regurgitation of food into the airways can lead to aspiration pneumonia, which occurs when food particles are inhaled into the lungs, causing an infection.
- Esophageal Cancer: In rare cases, chronic achalasia may increase the risk of developing esophageal cancer, particularly if it is left untreated over a long period.
- Food Impaction: Food can become stuck in the esophagus, leading to painful blockages and the need for emergency medical treatment.
How is Achalasia Cardia Diagnosed?
Achalasia cardia is diagnosed through a combination of clinical symptoms, physical examination, and various diagnostic tests. Common diagnostic procedures include:
(1) Barium Swallow X-ray
In this test, you drink a special liquid called barium that shows up on an X-ray. As it moves through your esophagus, the X-ray images help doctors see how your esophagus is working. In Achalasia Cardia, this test can show the “bird-beak” shape at the bottom of the esophagus, where the lower esophageal sphincter (LES) doesn’t relax properly, causing food to get stuck and the esophagus to widen.
(2) Esophageal Manometry
This test measures the pressure inside your esophagus. A small tube with sensors is placed into your esophagus, and you swallow small sips of water. The sensors check how well your esophagus and lower esophageal sphincter (LES) are working. In Achalasia, the LES doesn’t open when you swallow, and the muscles in your esophagus don’t work properly, making it hard to swallow food and liquids.
(3) Endoscopy (Gastroscopy)
In this procedure, a doctor uses a flexible tube with a camera to look directly at the inside of your esophagus. This helps them check for any problems like food stuck in the esophagus, inflammation, or signs of ulcers. For Achalasia, doctors might see food that hasn’t passed into the stomach because the esophagus isn’t working properly.
(4) High-Resolution Manometry (HRM):
This is a more advanced version of the manometry test. It uses a special device with multiple sensors to give a very detailed picture of how your esophagus is working. It can show exactly where the muscles aren’t moving properly and how the LES is behaving. This test helps doctors understand how severe your Achalasia Cardia is and which type you have, guiding the best treatment.
Treatment Options for Achalasia Cardia
The treatment for achalasia focuses on relieving symptoms and improving the patient’s ability to swallow. Treatment options include lifestyle changes, medications, and, in more severe cases, surgical interventions:
(1) Medications:
- Calcium Channel Blockers: These drugs relax the muscles of the lower esophagus, improving swallowing in some patients. They are often used for mild cases or as temporary relief.
- Nitrates: Nitrate medications can relax the lower esophageal sphincter, helping food move into the stomach.
- Botox Injections: Botulinum toxin (Botox) can be injected into the lower esophageal sphincter to relax the muscle and reduce the symptoms of achalasia, providing temporary relief.
(2) Pneumatic Dilation
Pneumatic dilation is a procedure in which a balloon is inserted into the esophagus and inflated at the level of the lower esophageal sphincter to force it open. This can help relieve symptoms by improving the flow of food into the stomach. It is often effective but may need to be repeated in some cases.
(3) Heller Myotomy
Heller myotomy is a surgical procedure in which the muscles of the lower esophageal sphincter are cut to allow easier passage of food into the stomach. This is considered the most effective treatment for achalasia, especially in cases where other treatments have failed. The procedure is often performed laparoscopically (minimally invasive surgery).
(4) Peroral Endoscopic Myotomy (POEM):
POEM is a newer, minimally invasive technique that involves making small incisions in the esophagus using an endoscope and cutting the muscles of the lower esophageal sphincter. It has shown promising results in treating achalasia and is considered an alternative to Heller myotomy.
(5) Esophageal Stent
In some cases, a stent (a small mesh tube) may be placed in the esophagus to help keep it open and allow food to pass into the stomach. This option is usually reserved for severe cases or when other treatments are not effective.
Why Choose Us?
Contact Us