Get Care
Inguinal Hernia
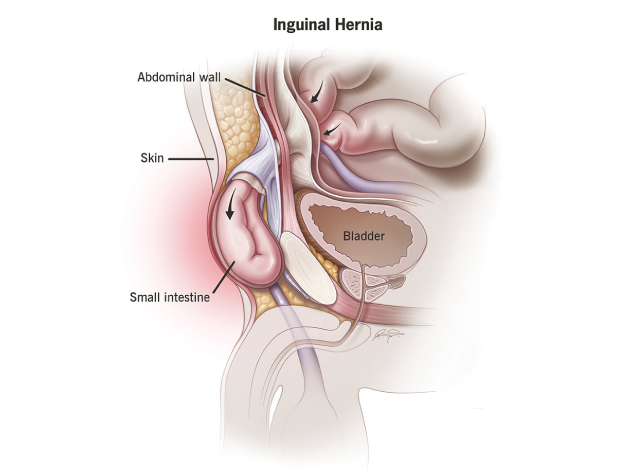
What is an Inguinal Hernia?
An inguinal hernia occurs when part of the intestine or other abdominal tissue pushes through a weakness or opening in the lower abdominal wall or the inguinal canal, which is a passage in the lower abdomen. This type of hernia is one of the most common types, especially in men, and can cause pain, discomfort, and other complications if left untreated. The hernia may present as a bulge in the groin or scrotum, which may become more prominent when lifting, coughing, or straining.
There are two primary types of inguinal hernias:
- Indirect Inguinal Hernia: This is the more common type and is often congenital (present at birth). The hernia follows the path of the inguinal canal, often descending into the scrotum in men. It occurs when the processus vaginalis, a structure in the abdomen that usually closes before birth, fails to close properly.
- Direct Inguinal Hernia: This type typically develops due to weakness in the abdominal wall, especially as a person ages. It does not follow the path of the inguinal canal, but protrudes directly through the abdominal wall into the inguinal region.
Inguinal Hernias can vary in size, from small and barely noticeable to large, and can sometimes be reducible (able to be pushed back in place) or incarcerated (trapped, unable to be pushed back).
What Causes an Inguinal Hernia?
An inguinal hernia occurs when abdominal contents—most commonly a portion of the intestine or fat—protrude through a weak spot in the lower abdominal wall near the inguinal canal. This condition arises due to a combination of structural weakness and increased intra-abdominal pressure.
(1) Congenital Defects (Indirect Inguinal Hernia)
In some individuals, the inguinal canal fails to close properly during fetal development. This leaves a persistent opening, which becomes a pathway for abdominal contents to protrude.
- This is the most common cause of indirect inguinal hernias, particularly in infants, children, and young adults.
- In males, the canal allows passage of the spermatic cord, and in females, the round ligament; if the canal remains open, herniation can easily occur.
(2) Increased Intra-Abdominal Pressure
A significant and chronic increase in pressure within the abdomen can push organs or tissues through areas of muscular weakness. Common causes include:
I. Heavy Lifting
Lifting heavy things the wrong way can strain your belly muscles, increasing pressure and making hernias more likely.
II. Chronic Coughing or Sneezing
Ongoing coughing from conditions like asthma or COPD puts repeated pressure on your abdomen, which can weaken muscles and cause hernias.
III. Straining During Bowel Movements or Urination
Problems like constipation or an enlarged prostate can make you strain often, which builds up pressure and wears out your abdominal wall.
IV. Obesity
Extra body weight adds constant pressure to your belly area and weakens the muscles, raising the risk of a hernia.
(3) Aging
- With age, connective tissues and muscles lose strength and elasticity.
- This natural degeneration weakens the abdominal wall and predisposes elderly individuals to direct inguinal hernias, which protrude through an acquired defect in the inguinal region.
(4) Previous Abdominal Surgery
- Surgical procedures, particularly those involving the lower abdomen, may weaken the integrity of the abdominal wall.
- Scar tissue and healing defects can create areas of vulnerability where hernias may eventually form.
(5) Gender (Male Predominance)
- Men are significantly more likely to develop inguinal hernias than women.
- This is due to the anatomical structure of the male inguinal canal, which is naturally larger and includes the spermatic cord, creating an area of relative weakness.
During fetal development, testes descend through the inguinal canal, leaving a potential space behind, making this site prone to herniation.
What are the Signs and Symptoms of an Inguinal Hernia?
Inguinal hernias often present with symptoms that can vary in severity and may sometimes be asymptomatic. The most common signs and symptoms include:
- Visible Bulge in the Groin or Scrotum: This bulge is usually more noticeable when standing, coughing, or straining. It may disappear or reduce in size when lying down.
- Pain or Discomfort: A dull ache or sharp pain may occur in the groin, especially during activities that increase abdominal pressure, such as lifting, coughing, or straining. The discomfort can worsen over time.
- Heaviness or Feeling of Dragging: A sensation of heaviness or dragging in the lower abdomen or groin, especially when standing or walking for long periods.
- Swelling or Enlargement of the Scrotum in Men: In cases of indirect inguinal hernias, the bulge may extend into the scrotum.
- Burning or Aching Sensation: Some individuals report a burning or aching feeling at the hernia site.
- Nausea and Vomiting: These symptoms may occur if the hernia causes an intestinal obstruction.
What are the Risk Factors for Inguinal Hernia?
While anyone can develop an inguinal hernia, several factors increase the likelihood:
- Male Gender: Men are more likely to develop inguinal hernias due to the anatomical structure of the inguinal canal.
- Age: The risk increases with age, as abdominal wall muscles weaken over time.
- Family History: A genetic predisposition to hernias may exist, especially if close family members have had hernias.
- Obesity: Excess weight increases pressure on the abdominal wall, making hernias more likely.
- Chronic Cough: Conditions like chronic bronchitis or asthma that cause frequent coughing can increase abdominal pressure.
- Heavy Lifting: Individuals who engage in lifting heavy objects, especially without proper technique, are at higher risk.
- Constipation: Chronic constipation and straining during bowel movements place pressure on the abdominal wall.
- Previous Abdominal Surgery: Scar tissue from prior surgeries can weaken the abdominal wall.
What are the Complications of an Inguinal Hernia?
If left untreated or if complications arise, an inguinal hernia can lead to severe health issues:
- Incarceration: When the hernia becomes trapped, it cannot be pushed back into the abdomen. This can cause bowel obstruction and pain.
- Strangulation: When the blood supply to the herniated tissue is cut off, it can lead to tissue death (necrosis), resulting in gangrene. This is a medical emergency requiring immediate surgery.
- Bowel Obstruction: Protruding intestine or fatty tissue may block the intestines, leading to severe pain, vomiting, and inability to pass stools or gas.
- Infertility in Men: In rare cases, a large inguinal hernia that extends into the scrotum may cause pressure on the spermatic cord, potentially leading to infertility.
- Recurring Hernia: Even after surgical repair, a hernia can reappear, particularly if the underlying cause isn’t addressed.
Diagnosis of Inguinal Hernia
Diagnosing an inguinal hernia involves a combination of clinical evaluation and imaging techniques, particularly in complex or recurrent cases. Early and accurate diagnosis is crucial to prevent complications such as incarceration or strangulation.
(1) Physical Examination (Primary Diagnostic Method)
The clinical examination is the most important and commonly used step in diagnosing an inguinal hernia.
- The patient is usually asked to stand upright, as this position increases intra-abdominal pressure and makes the hernia more visible.
- The healthcare provider will inspect and palpate the groin area, particularly around the inguinal canal.
- The patient may be asked to cough or strain (Valsalva maneuver), which can provoke a bulge or protrusion of the hernia, confirming its presence.
- The examiner will also evaluate:
- Whether the bulge is reducible (able to be pushed back into the abdomen)
- The size and consistency of the protrusion
- Tenderness or signs of complications such as pain, redness, or heat
In men, the examiner may insert a finger into the inguinal canal via the scrotum to feel for herniation along the spermatic cord.
(2) Hernia Push Test (Reducibility Assessment)
This is a simple manual technique used during the physical exam to determine the type and severity of the hernia.
- The physician gently presses on the hernia bulge to see if it can be pushed back into the abdomen.
- A reducible hernia usually presents with minimal pain and can be pushed back easily.
- An incarcerated hernia cannot be reduced and may feel firm or tender, suggesting a trapped segment of intestine or fat.
- If the hernia is strangulated (blood supply cut off), it will be extremely painful, swollen, and possibly discolored — requiring emergency surgery.
(3) Ultrasound Imaging
Ultrasound is often the first-line imaging test when the diagnosis is uncertain or the hernia is not easily visible.
- It is non-invasive, radiation-free, and suitable for all ages.
- Helps confirm the presence of a hernia sac and determine its size, contents, and exact location.
- Especially useful in pediatric cases, in obese patients, or when a femoral hernia (near the thigh) is suspected.
- Can also help detect complications such as bowel obstruction or compromised blood flow.
(4) CT Scan (Computed Tomography)
A CT scan provides a detailed cross-sectional view of the abdomen and pelvic region.
- Used when the hernia is recurrent, complex, or not clearly palpable.
- Useful for identifying multiple hernias, hidden defects, or intra-abdominal pathology.
- Can detect complications like obstruction, strangulation, or adhesions in patients with previous surgeries.
(5) MRI (Magnetic Resonance Imaging)
MRI is less commonly used but may be indicated in difficult-to-diagnose cases or when soft tissue contrast is important.
- Provides detailed imaging without radiation.
- Ideal for athletes with groin pain when a hernia is suspected but not confirmed by ultrasound or CT.
- Helpful in distinguishing hernias from other soft tissue masses or inguinal canal abnormalities.
Treatment of Inguinal Hernia
Surgical repair is the only effective treatment for an inguinal hernia. Treatment may be required if the hernia is causing symptoms or has a risk of becoming incarcerated or strangulated.
Surgical Options:
- Open Hernia Repair: This is the most traditional method, where a surgeon makes an incision in the groin to return the hernia contents to the abdomen and repair the defect using a synthetic mesh to reinforce the abdominal wall. The mesh reduces the likelihood of the hernia recurring.
- Laparoscopic Hernia Repair: This minimally invasive procedure involves smaller incisions and the use of a camera to guide the surgeon. A mesh is inserted to repair the hernia. This technique offers faster recovery, less postoperative pain, and smaller scars.
- Robotic-assisted Surgery: A more advanced form of laparoscopic surgery, robotic-assisted surgery provides the surgeon with enhanced precision, particularly in complex hernias.
- Hernia Surgery in Infants/Children: In younger patients, a small incision is made to repair the hernia, which may resolve without a mesh in some cases.
Lifestyle and Preventive Measures
Preventing an inguinal hernia primarily involves reducing the risk factors that contribute to its development:
- Maintain a healthy weight: Avoid excess abdominal pressure caused by obesity.
- Avoid heavy lifting: Lift objects properly, using the legs rather than the back and avoiding excessive weight.
- Treat constipation: Ensure regular bowel movements and use stool softeners if necessary to prevent straining.
- Quit smoking: Smoking weakens connective tissue, increasing the likelihood of hernias.
- Proper posture: Prevent unnecessary strain on the abdominal wall by maintaining good posture, especially while standing or sitting for long periods.
Prognosis
With timely diagnosis and appropriate surgical intervention, the prognosis for inguinal hernia repair is excellent. Most patients experience minimal postoperative pain and return to regular activities within 2 to 4 weeks. The recurrence rate is low with modern surgical techniques, especially when mesh is used.
Why Choose Us?
Contact Us