Get Care
Umbilical Hernia
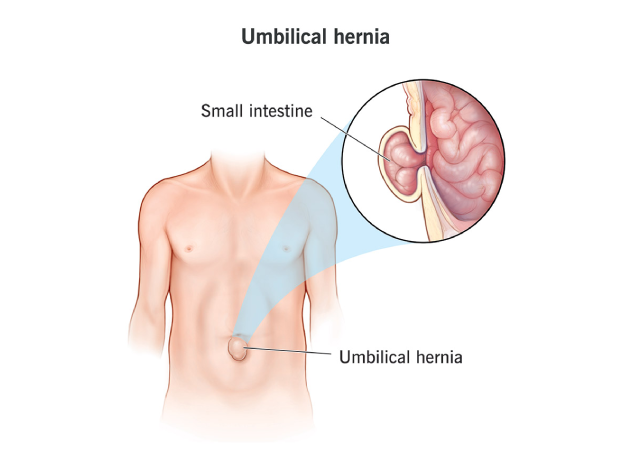
What is an Umbilical Hernia?
An umbilical hernia occurs when a part of the intestine or abdominal tissue bulges through a weak spot in the abdominal muscles near the belly button (umbilicus). This condition is more common in infants but can also occur in adults. In adults, it is often associated with increased abdominal pressure, obesity, pregnancy, or a history of surgery.Umbilical hernias in infants are usually congenital, meaning they are present at birth, and are typically seen as a small bulge at the navel area. In adults, the hernia may develop as a result of increased pressure on the abdominal wall, and the bulge may become more prominent during activities such as lifting, coughing, or straining.
What Causes an Umbilical Hernia?
Umbilical hernias are caused by a weakness or opening in the abdominal muscles near the belly button. The reasons for this weakness vary depending on the individual:
- Congenital Factors (in Infants): During fetal development, the muscles around the belly button do not fully close, leaving a small opening. If this opening does not close properly after birth, it can allow part of the intestine or fatty tissue to push through, forming a hernia.
- Increased Abdominal Pressure (in Adults): Conditions that increase pressure in the abdomen, such as pregnancy, obesity, chronic coughing, heavy lifting, or constipation, can lead to the development of an umbilical hernia.
- Weakening of Abdominal Muscles (in Adults): Age, prior surgeries, or conditions like ascites (fluid buildup in the abdomen) can weaken the abdominal muscles, making them more prone to hernias.
- Congenital Factors (in Infants): During fetal development, the muscles around the belly button do not fully close, leaving a small opening. If this opening does not close properly after birth, it can allow part of the intestine or fatty tissue to push through, forming a hernia.
What are the Signs and Symptoms of an Umbilical Hernia?
An umbilical hernia often presents with the following symptoms:
- Visible Bulge: A small bulge or lump near the belly button is the hallmark sign of an umbilical hernia. This bulge may become more noticeable when coughing, crying, or straining and may disappear or reduce in size when lying down.
- Pain or Discomfort: A mild ache or pain at the site of the hernia, especially when coughing or lifting heavy objects. In most cases, the hernia is painless, but pain may occur if the hernia becomes incarcerated or strangulated.
- Tenderness: The area around the bulge may be tender to the touch, particularly in adults or when the hernia becomes larger.
- No Symptoms in Some Cases: In many cases, especially in infants, the hernia may be painless and may not cause any symptoms other than a visible bulge.
What are the Risk Factors for Umbilical Hernia?
Several factors can increase the likelihood of developing an umbilical hernia:
- Age: Umbilical hernias are most common in infants but can also occur in adults, particularly in those over the age of 40.
- Obesity: Being overweight or obese increases pressure on the abdominal wall, making it more likely to develop a hernia.
- Multiple Pregnancies: Pregnancy can stretch and weaken the abdominal muscles, increasing the risk of developing a hernia.
- Chronic Coughing: Conditions such as chronic bronchitis, asthma, or other respiratory conditions that lead to frequent coughing can increase abdominal pressure.
- Previous Surgery: If someone has had abdominal surgery, scar tissue or weakened muscles may create a potential site for a hernia.
- Family History: A family history of hernias can increase the likelihood of developing an umbilical hernia.
- Ascites: Fluid buildup in the abdomen (ascites) can put added pressure on the abdominal wall, leading to a hernia.
What are the Complications for Umbilical Hernia?
While most umbilical hernias are not dangerous, complications can arise, particularly in adults:
- Incarceration: The hernia becomes stuck, and the contents (usually part of the intestine) cannot be pushed back into the abdomen. This can lead to pain, swelling, and potential obstruction of the intestines.
- Strangulation: This occurs when the blood supply to the herniated tissue is cut off, leading to tissue death (gangrene). This is a medical emergency and requires immediate surgical intervention.
- Bowel Obstruction: If the intestine becomes trapped in the hernia, it can lead to a blockage in the bowel, causing severe pain, nausea, vomiting, and inability to pass stool or gas.
Diagnosis of Umbilical Hernia
An umbilical hernia occurs when part of the intestine, fat, or fluid pushes through a weakness in the abdominal muscles at or near the belly button (umbilicus). The diagnosis is typically straightforward and primarily made based on clinical examination. In select or complicated cases, imaging tests may be necessary for confirmation or further evaluation.
(1) Clinical Diagnosis (Primary Method)
The physical examination is the cornerstone of diagnosing an umbilical hernia. This is often sufficient to confirm the presence and assess the severity of the hernia.
What to Expect During the Exam:
- The patient is usually examined in both standing and lying down positions.
- The doctor looks for a visible or palpable bulge at the umbilicus.
- The hernia may become more prominent when the patient coughs, strains, or stands, as these actions increase intra-abdominal pressure.
- In infants, the hernia is often visible when the baby cries or coughs.
- The examiner checks whether the bulge is:
- Reducible (can be gently pushed back into the abdomen)
- Irreducible (fixed, suggesting incarceration)
- Tender, firm, or discolored (may indicate strangulation — a medical emergency)
In many adults and children, a small, soft, and reducible hernia is easily diagnosed without the need for further testing.
(2) Imaging Tests (For Unclear or Complicated Cases)
While imaging is not routinely required, it plays an important role in atypical presentations, when the diagnosis is uncertain, or when complications such as incarceration or strangulation are suspected.
I. Ultrasound
- A non-invasive and safe imaging tool, especially useful in children and pregnant women.
- Helps in identifying small or occult hernias not easily seen during a physical exam.
- Assesses the hernia sac contents, whether bowel loops or fat, and detects signs of incarceration or lack of blood flow.
II. CT Scan (Computed Tomography)
- Provides a detailed cross-sectional view of the abdominal wall and contents.
- More often used in adults to evaluate:
- Large or recurrent hernias
- Multiple abdominal wall defects
- Suspected complications like obstruction or strangulation
- Especially helpful when the hernia is not externally obvious or if there’s abdominal pain of unclear origin.
III. MRI (Rare Use)
- May be used in complex cases or when soft tissue differentiation is necessary.
- Occasionally used to distinguish hernias from other abdominal wall masses or to assess associated muscular issues.
(3) Diagnosis in Infants and Children
- In newborns and infants, the diagnosis is almost always clinical.
- The hernia often appears as a soft bulge near the navel that becomes more prominent when the child cries.
Pediatric hernias are usually painless and reducible, and most close spontaneously by age 3–5 years.
Treatment of Umbilical Hernia
In many cases, especially in infants, an umbilical hernia may resolve on its own as the abdominal muscles grow stronger. However, if the hernia persists or causes symptoms in adults, surgery may be necessary.
Surgical Treatment:
The standard treatment for an umbilical hernia is surgery to repair the hole in the abdominal wall. The surgery may involve:
- Hernia Repair Surgery (Herniorrhaphy): This is a relatively simple procedure where the surgeon makes an incision near the belly button, pushes the hernia back into place, and repairs the weakened muscle with sutures. Sometimes, a mesh is used to reinforce the abdominal wall.
- Laparoscopic Surgery: This minimally invasive procedure involves smaller incisions and the use of a camera to guide the surgeon. Laparoscopic surgery typically results in less postoperative pain and a faster recovery time.
Surgery is generally recommended for adults or for children whose hernia does not resolve on its own by the age of 3 to 5 years. Emergency surgery is required if complications such as incarceration or strangulation occur.
Lifestyle and Supportive Measures
For adults, there are several measures to help manage and reduce the risk of worsening an umbilical hernia:
- Avoid Straining: Try to avoid activities that increase abdominal pressure, such as heavy lifting or straining during bowel movements.
- Maintain a Healthy Weight: Achieving and maintaining a healthy weight helps reduce pressure on the abdominal wall.
- Treat Chronic Cough: If you have a persistent cough, it’s important to treat the underlying cause, whether it’s related to smoking, asthma, or another respiratory condition.
- Manage Constipation: If constipation is an issue, use fiber supplements or stool softeners to avoid straining during bowel movements.
- Follow-up with Your Doctor: Regular check-ups with your healthcare provider are essential to monitor the hernia and determine if surgical intervention is necessary.
Prognosis
Most people with an umbilical hernia can expect a positive outcome with treatment. For infants, the hernia usually resolves on its own within the first year of life. In adults, surgical repair is highly effective, with most individuals returning to normal activities within a few weeks. The risk of recurrence is low, especially with modern surgical techniques involving mesh reinforcement.
Why Choose Us?
Contact Us