Get Care
Appendicitis
What is Appendicitis?
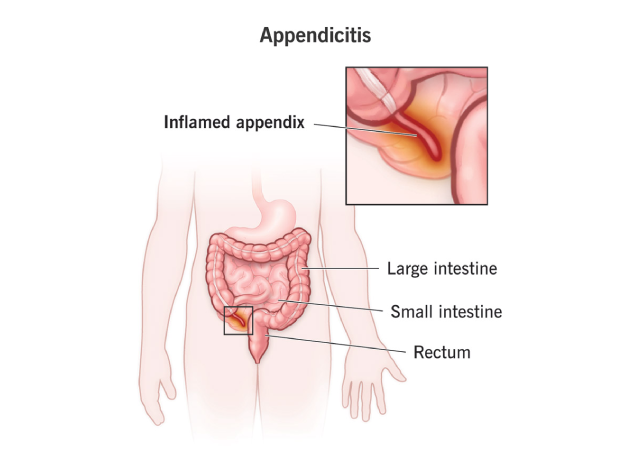
Appendicitis is the inflammation and infection of the appendix, a small, finger-shaped organ located at the junction of the small and large intestines, specifically in the lower right side of the abdomen. Though its function is not entirely clear, the appendix is considered a vestigial organ, possibly involved in gut immunity.
Appendicitis is one of the most common surgical emergencies worldwide. If not treated in time, the inflamed appendix may burst, leading to a serious and potentially fatal infection of the abdominal cavity, known as peritonitis. Early recognition and prompt surgical removal of the appendix (appendectomy) are essential to prevent complications.
What are the Causes of Appendicitis?
Appendicitis usually results from an obstruction in the lumen (opening) of the appendix. This blockage can be due to:
Fecaliths (hardened stool) – most common cause
Enlarged lymphoid tissue due to a gastrointestinal or respiratory infection
Parasitic infestations
Foreign bodies
Tumors (rare)
Trauma to the abdomen
The obstruction allows bacteria to multiply within the appendix, causing it to swell. As pressure builds, blood flow is reduced, leading to tissue death, rupture, and spread of infection within the abdomen.
What are the Signs and Symptoms of Appendicitis?
The symptoms of appendicitis can vary depending on the patient’s age and the position of the appendix, but typical features include:
Abdominal pain: This often begins around the navel (periumbilical region) and shifts to the lower right side (right iliac fossa) within a few hours. The pain increases in intensity and may become sharp and localized.
Loss of appetite: One of the earliest and most consistent symptoms.
Nausea and vomiting: Usually follow the onset of pain.
Fever: A low-grade fever is common in early stages. A higher temperature may indicate rupture.
Constipation or diarrhea: Some patients may experience either, along with gas retention.
Abdominal bloating: More prominent in children or in cases with delayed diagnosis.
Pain with movement: Pain worsens with coughing, walking, or any jarring movements.
Rebound tenderness: Pain intensifies when pressure applied to the lower abdomen is suddenly released.
Rovsing’s sign: Pain in the right lower abdomen when the left side is palpated.
Atypical presentations are common in:
Children: May present with only vomiting and lethargy.
Elderly: Symptoms may be less pronounced, leading to delayed diagnosis.
Pregnant women: The location of the appendix is shifted upward, which can cause confusion with other abdominal conditions.
What are the Risk Factors for Appendicitis?
While appendicitis can occur in individuals of all ages and backgrounds, certain factors may increase the likelihood of developing this condition. Understanding these risk factors can help in early detection and timely medical intervention:
Age: Most common between 10–30 years.
Gender: Slightly more frequent in males.
Family History: A genetic predisposition may exist in families.
Low-Fiber Diet: Diets low in fiber and high in processed foods can lead to stool blockages (fecaliths).
Infections: Gastrointestinal or respiratory infections may cause swelling of lymph tissue that blocks the appendix.
Cystic Fibrosis: Thick mucus can obstruct the appendix.
Chronic Gut Conditions: Inflammatory bowel diseases like Crohn’s may increase risk.
Early recognition of these factors helps in timely diagnosis and treatment, reducing the chance of complications.
What are the Complications of Appendicitis?
If not treated promptly, appendicitis can lead to:
Perforation (rupture) of the appendix: Causes spillage of infected material into the abdominal cavity.
Peritonitis: A life-threatening infection and inflammation of the peritoneal lining.
Appendicular abscess: A localized collection of pus near the appendix.
Appendicular mass (phlegmon): Inflamed appendix surrounded by fat and bowel loops.
Sepsis: A systemic infection that can cause multi-organ failure.
Bowel obstruction: Inflammation may affect nearby intestines.
Complications significantly increase morbidity and hospital stay, especially when diagnosis is delayed.
What are the Diagnosis of Appendicitis?
Diagnosis of appendicitis is primarily based on clinical evaluation but is often supported by laboratory tests and imaging studies to improve accuracy and rule out other conditions. The diagnostic process typically includes the following steps:
- Physical Examination:
The doctor checks for signs of localized tenderness, especially at McBurney’s point (a spot in the lower right abdomen). Additional signs include:- Rebound tenderness: Pain when pressure is suddenly released.
- Guarding: Tensing of abdominal muscles in response to touch.
- Rovsing’s sign: Pain in the right lower abdomen when the left side is pressed.
- Psoas sign: Pain when the patient extends the right thigh, indicating irritation of the psoas muscle.
- Blood Tests:
These are used to detect signs of infection and inflammation:- Elevated white blood cell (WBC) count (leukocytosis).
- Increased C-reactive protein (CRP) levels.
- Urinalysis:
Helps exclude other conditions such as urinary tract infections (UTIs) or kidney stones, which can mimic appendicitis symptoms. - Ultrasound of the Abdomen:
Commonly used in children and pregnant women due to the absence of radiation. It can help visualize an inflamed appendix and detect complications like an abscess. - CT Scan of the Abdomen:
Considered the preferred imaging method in adults. It has high accuracy in diagnosing appendicitis and can also identify complications such as perforation or abscess formation. - MRI (Magnetic Resonance Imaging):
An alternative imaging technique, especially useful in pregnant women, as it avoids radiation exposure while still providing detailed images.
What is the Treatment for Appendicitis?
The mainstay of treatment for appendicitis is surgical removal of the appendix (appendectomy). The approach may vary based on the stage of the disease.
- Surgical Treatment:
- Laparoscopic appendectomy – Minimally invasive, faster recovery
- Open appendectomy – Preferred in cases of perforation, abscess, or difficult anatomy
- Non-surgical (Conservative) Management:
- In selected cases of uncomplicated appendicitis, antibiotics may be used as initial therapy.
- Reserved for high-risk surgical candidates or those refusing surgery.
- However, recurrence is common with non-surgical management.
- Management of Complicated Appendicitis:
- In cases of abscess or phlegmon, initial treatment with IV antibiotics and drainage (if needed), followed by interval appendectomy after 6–8 weeks.
- In cases of abscess or phlegmon, initial treatment with IV antibiotics and drainage (if needed), followed by interval appendectomy after 6–8 weeks.
Postoperative Care and Recovery
- Most patients recover within 1–2 weeks after laparoscopic appendectomy.
- Early ambulation, pain control, and wound care are essential.
- Activity restrictions and dietary modifications may be advised briefly.
- Monitoring for signs of infection, such as fever, redness, or discharge from the incision site, is necessary.
Why Choose Us?
Contact Us