Get Care
CA Rectum (Rectal Cancer)
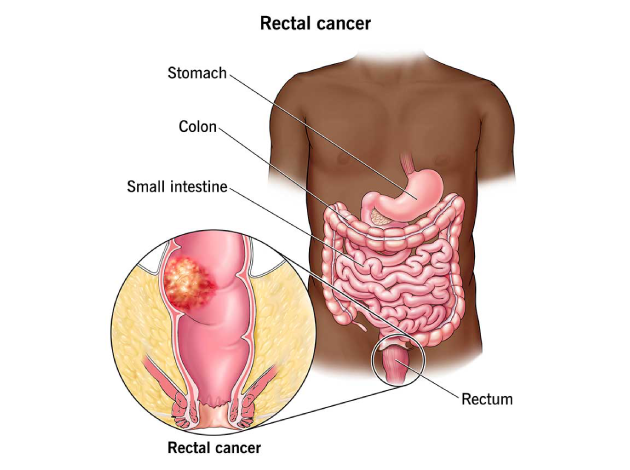
What is Rectal Cancer (CA Rectum)?
Rectal cancer is a type of cancer that arises in the rectum—the final portion of the large intestine, located just above the anal canal. It typically begins as abnormal growths known as polyps, which can become malignant over time. While rectal cancer is often grouped with colon cancer as part of colorectal cancer, it has distinct anatomical, surgical, and treatment considerations due to its proximity to the anal sphincter and surrounding pelvic structures.The rectum plays a critical role in stool storage and continence. As such, tumors in this area can significantly affect a person’s bowel habits, continence, and quality of life. Early detection and a multidisciplinary approach to treatment are essential for optimal outcomes.
What Causes Rectal Cancer?
Rectal cancer develops when cells in the rectal lining undergo genetic mutations that disrupt normal cell growth, leading to tumor formation. While the exact cause is often unclear, several key factors contribute:
(1) Adenomatous Polyps
Most rectal cancers start as benign polyps that gradually become cancerous over time.
(2) Chronic Inflammation
Conditions like ulcerative colitis and Crohn’s disease increase risk through repeated tissue damage and repair.
(3) Inherited Syndromes
Genetic conditions like Lynch Syndrome and Familial Adenomatous Polyposis (FAP) greatly raise lifetime cancer risk.
(4) Sporadic Mutations & Lifestyle
Aging, poor diet (high red meat, low fiber), smoking, obesity, and alcohol use can all lead to mutations that trigger cancer.
Symptoms of Rectal Cancer
Symptoms may overlap with those of hemorrhoids or other anorectal conditions, making early diagnosis challenging. Key symptoms include:
- Rectal bleeding – bright red blood or blood-streaked stools
- Change in bowel habits – persistent constipation or diarrhea
- Tenesmus – a feeling of incomplete bowel evacuation
- Narrow-caliber stools (“pencil-thin” stool)
- Unexplained weight loss
- Abdominal discomfort or cramping
- Mucus in stools
- Fatigue and weakness (from anemia)
- In advanced cases: bowel obstruction or fistula formation
What are the Risk Factors for Rectal Cancer?
Risk factors are similar to those for colon cancer and include :
Age
– Most cases occur in people over 50, though it can affect younger individuals.Family History
– A family history of colorectal cancer or polyps increases risk, especially if diagnosed at a young age.Inherited Syndromes
– Conditions like Lynch Syndrome and Familial Adenomatous Polyposis (FAP) significantly increase the risk.Personal History of Polyps or Cancer
– Previous colorectal cancer or adenomatous polyps raise the chances of recurrence.Inflammatory Bowel Disease (IBD)
– Long-standing ulcerative colitis or Crohn’s disease increases cancer risk due to chronic inflammation.Diet
– Diets high in red or processed meat and low in fiber are linked to higher cancer risk.Lifestyle Factors
– Obesity, physical inactivity, smoking, and heavy alcohol use all contribute to increased risk.Type 2 Diabetes
– Associated with a modestly elevated risk, possibly due to insulin resistance.Radiation Therapy
– Prior radiation to the pelvic area may raise rectal cancer risk.
What are the Complications of Rectal Cancer?
Bowel Obstruction
– Tumors can block the rectum or colon, causing pain, bloating, constipation, and vomiting.Bleeding and Anemia
– Chronic blood loss from the tumor may lead to iron-deficiency anemia, resulting in fatigue and weakness.Perforation of the Bowel
– In rare cases, the cancer can cause a hole in the bowel wall, leading to life-threatening infection (peritonitis).Fistula Formation
– Abnormal connections (fistulas) may develop between the rectum and nearby organs like the bladder or vagina.Incontinence
– Cancer or its treatment may damage the nerves or muscles that control bowel movements.Metastasis
– Cancer can spread (metastasize) to the liver, lungs, or other organs, making treatment more complex and prognosis worse.Sexual and Urinary Dysfunction
– Especially after pelvic surgery or radiation, nerves affecting bladder or sexual function may be damaged.Psychological Effects
– Living with rectal cancer can cause depression, anxiety, and body image concerns, particularly after surgeries like colostomy.
Diagnosis of Rectal Cancer
Diagnosing rectal cancer accurately requires a comprehensive evaluation that combines clinical examination, endoscopic procedures, imaging studies, and laboratory tests. These methods help detect the presence of cancer, determine its location, assess the extent of local and distant spread, and guide treatment planning.
(1) Digital Rectal Examination (DRE)
The diagnostic process often begins with a digital rectal examination, where a doctor inserts a gloved, lubricated finger into the rectum to feel for any abnormal masses, irregularities, or thickening of the rectal wall. This simple exam can detect tumors in the lower rectum and is an important initial step in identifying suspicious findings.
(2) Endoscopic Evaluation
- Proctoscopy and Colonoscopy are key tools that allow direct visualization of the inside of the rectum and colon. During these procedures, a flexible tube with a camera is inserted into the rectum to inspect for tumors, polyps, bleeding, or inflammation.
- If a suspicious lesion is found, a biopsy (tissue sample) is taken and sent for histopathological examination to confirm the presence of cancer and determine its grade and type.
(3) Carcinoembryonic Antigen (CEA) Test
CEA is a tumor marker that may be elevated in some patients with rectal cancer. While it is not used for diagnosis alone, it plays a valuable role in:
- Monitoring treatment response
- Detecting recurrence after treatment
High levels of CEA before treatment may also indicate a more aggressive disease.
(4) Imaging for Local and Distant Assessment
Imaging studies are essential to determine how far the cancer has spread, both locally within the pelvis and to distant organs.
I. Pelvic MRI (Magnetic Resonance Imaging)
Pelvic MRI is the most important imaging tool for local staging. It provides detailed images of:
- The depth of tumor invasion into the rectal wall
- Involvement of surrounding tissues (such as the sphincter muscles)
- Nearby lymph node involvement
This helps decide whether surgery alone is sufficient or if chemotherapy/radiation is needed first.
II. CT Scan of the Chest, Abdomen, and Pelvis
A CT scan evaluates whether the cancer has spread (metastasized) to distant organs, particularly the liver and lungs, which are the most common sites for metastasis in rectal cancer. It is crucial for comprehensive staging and treatment planning.
III. Endorectal Ultrasound (ERUS)
ERUS uses a specialized ultrasound probe inserted into the rectum to assess:
- The depth of tumor penetration into the rectal wall layers
- Nearby lymph node involvement
It is particularly useful in early-stage rectal cancers for fine assessment of local tumor invasion.
Treatment of Rectal Cancer
Treatment requires careful planning due to the anatomical constraints of the pelvis and the goal of preserving anal function. Options include:
(1) Surgery (mainstay of treatment):
- Low Anterior Resection (LAR): For upper and mid-rectal tumors, preserving sphincter
- Abdominoperineal Resection (APR): For low rectal tumors involving sphincter, resulting in permanent colostomy
- Local excision or transanal endoscopic microsurgery (TEM): For early-stage, small tumors
(2) Neoadjuvant Therapy (before surgery):
Chemoradiation (CRT): Standard for Stage II & III to shrink tumor, improve resectability, and reduce recurrence
(3) Adjuvant Chemotherapy (after surgery):
Recommended in Stage III or high-risk Stage II
Common regimens include FOLFOX or CAPOX
(4) Targeted Therapy and Immunotherapy (in selected metastatic cases):
Used when tumors express specific markers (e.g., MSI-H)
(5) Palliative care:
For advanced cases to manage symptoms and improve quality of life
Lifestyle and Supportive Measures
- Regular screenings (colonoscopy) starting at age 45 or earlier in high-risk individuals
- High-fiber diet, low in red/processed meat
- Physical activity and healthy weight maintenance
- Smoking cessation and limiting alcohol
- Psychosocial support and rehabilitation (especially for stoma care or sexual dysfunction)
- Routine follow-ups post-treatment to detect recurrence
Prognosis
Prognosis depends on the stage at diagnosis, response to treatment, and overall patient health. Early-stage rectal cancer has a 5-year survival rate of over 80–90%, while survival decreases significantly with advanced disease or distant metastasis. Preoperative chemoradiation has improved outcomes and reduced local recurrence rates significantly.
Why Choose Us?
Contact Us