Get Care
Fistula-in-Ano
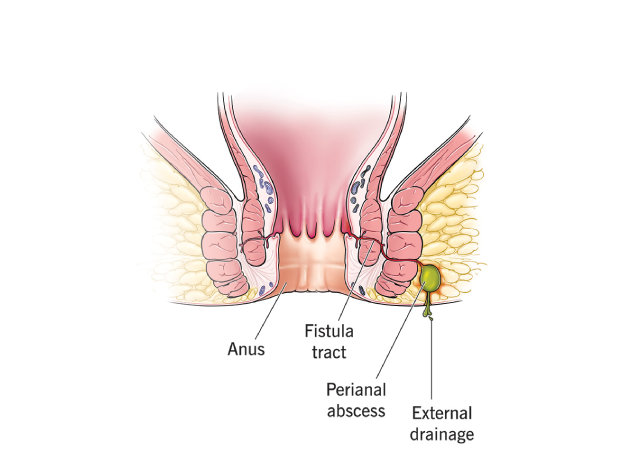
What is Fistula-in-Ano?
What Causes Fistula-in-Ano?
The primary cause of fistula-in-ano is an anal abscess. The infection from the abscess forms a tract or tunnel that connects the infected gland inside the anus to the skin outside. Other possible causes and risk factors include:
- Infections: Anal abscesses are the most common cause of fistula formation. The infection usually starts in one of the anal glands, which can become blocked and infected.
- Inflammatory Bowel Disease (IBD): Conditions such as Crohn’s disease or ulcerative colitis can lead to the formation of fistulas due to chronic inflammation in the gastrointestinal tract.
- Trauma: Injury or surgery to the anal area may cause scarring or an infection that leads to a fistula.
- Cancer: Although rare, anal or colorectal cancers can cause fistulas to form as the cancer spreads and invades surrounding tissues.
- Sexually Transmitted Infections (STIs): Some infections, such as syphilis, tuberculosis, and HIV, can cause fistulas to form in the anal region.
- Chronic constipation or straining: Long-term pressure or straining on the anal region can increase the risk of infection and subsequent fistula formation.
What are the Symptoms of Fistula-in-Ano?
The symptoms of fistula-in-ano can vary depending on the type and severity of the condition. Common symptoms include:
- Pain or discomfort around the anus, especially during or after bowel movements.
- Persistent or intermittent drainage from an opening near the anus. The drainage may be clear, cloudy, or may contain pus or blood.
- Itching or irritation around the anus.
- Redness or swelling near the anal opening.
- Foul-smelling discharge from the opening of the fistula.
- Recurrent abscesses in the same area.
- Fever and chills (in severe cases, if there is an associated infection).
In some cases, people with fistula-in-ano may also experience symptoms related to an underlying condition such as Crohn’s disease, including diarrhoea, weight loss, or abdominal discomfort.
What are the Risk Factors for Fistula-in-Ano?
Certain factors may increase the risk of developing a fistula-in-ano, including:
- Previous Anal Abscess: Having an anal abscess is the most common risk factor for developing a fistula-in-ano.
- Inflammatory Bowel Disease (IBD): People with conditions such as Crohn’s disease are at higher risk of developing anal fistulas due to chronic inflammation.
- Diabetes: Poorly controlled diabetes can impair the immune system and increase the risk of infections, including anal abscesses.
- Trauma or Surgery: Injury to the anal region or previous anal surgeries can lead to scarring and the formation of fistulas.
- HIV: Individuals with HIV are more prone to infections, including those that lead to fistula formation.
What are the Complications of Fistula-in-Ano?
If left untreated, fistula-in-ano can lead to several complications:
- Chronic Infection: The fistula can become infected repeatedly, leading to abscesses and worsening symptoms.
- Abscess Formation: The presence of a fistula often leads to the formation of an anal abscess, which can be extremely painful and require surgical drainage.
- Incontinence: In rare cases, if the fistula becomes large or involves the anal sphincter muscles, it can lead to fecal incontinence (inability to control bowel movements).
- Skin Irritation: Continuous drainage of pus or fecal material can irritate the surrounding skin.
- Recurrence: Fistulas can recur after treatment, especially if not properly managed or if there are underlying conditions like Crohn’s disease.
Diagnosis of Fistula-in-Ano
Fistula-in-ano is a chronic abnormal tunnel that forms between the anal canal and the skin near the anus, often following an anal abscess. Accurate diagnosis is crucial for effective treatment and to prevent recurrence. Diagnosis typically involves a combination of careful clinical examination and advanced imaging techniques to assess the fistula’s path, depth, and relationship to sphincter muscles.
(1) Medical History and Symptom Review
The diagnostic process begins with a detailed patient history. Common symptoms reported include:
- Persistent or intermittent pain, especially during bowel movements
- Swelling, redness, or tenderness around the anus
- Drainage of pus or stool-like material from an opening near the anus
- Recurrent anal abscesses
- Fever or malaise (in the case of infection)
A history of conditions like Crohn’s disease, tuberculosis, or previous perianal abscesses is also noted, as they increase the likelihood of a fistula.
(2) Physical Examination
A thorough visual and digital rectal examination is typically the first step:
- The healthcare provider inspects the perianal region for any external opening, redness, or signs of discharge.
- Palpation may reveal an indurated (hardened) tract under the skin.
- A digital rectal examination (DRE) is performed to detect any internal opening or associated in-duration along the anal canal.
- Gentle probing of the external opening may help identify the direction and depth of the tract but is done cautiously to avoid creating false tracts.
(3) Anoscopy
An anoscope, a short tube with a light, is used to examine the anal canal and rectum:
- This helps locate the internal opening of the fistula, particularly when not apparent on physical exam.
- Anoscopy is especially useful when paired with gentle probing to trace the fistula’s internal and external openings.
(4) Imaging Techniques
Imaging plays a vital role in evaluating the extent and complexity of the fistula:
I. MRI (Magnetic Resonance Imaging)
- Gold standard for diagnosing fistula-in-ano.
- Provides detailed, high-resolution images of soft tissues, showing:
- The path of the fistula
- Any secondary tracts
- Involvement of anal sphincter muscles
- Presence of abscesses or inflammation
- Particularly useful for complex or recurrent fistulas, or when sphincter-preserving surgery is planned.
II. Endorectal Ultrasound
- Involves inserting a specialised ultrasound probe into the rectum.
- Offers a cross-sectional view of the anal sphincters and fistula tract.
- Effective in identifying low-lying fistulas, especially in experienced hands.
III. Fistulogram
- An older technique, now less commonly used.
- A contrast dye is injected into the external fistula opening, followed by X-rays to visualise the tract.
- May be helpful in simple, superficial fistulas but has largely been replaced by MRI.
(5) Proctoscopy or Sigmoidoscopy
- These endoscopic procedures are done to examine the rectum and lower colon.
- Help identify any underlying conditions such as:
- Crohn’s disease
- Diverticulitis
- Colorectal cancer
- Particularly useful when symptoms suggest broader gastrointestinal involvement.
Treatment of Fistula-in-Ano
Treatment for fistula-in-ano aims to resolve the infection, heal the fistula, and prevent recurrence. Treatment options depend on the type and complexity of the fistula:
(1) Conservative Management:
- Antibiotics: These may be prescribed to treat any infection associated with the fistula, especially if an abscess is present.
- Pain Management: Pain relievers such as acetaminophen or ibuprofen can help manage discomfort.
- Sitz Baths: Soaking the affected area in warm water for 15–20 minutes several times a day can help reduce pain and promote healing.
(2) Surgical Treatment:
Surgery is the mainstay of treatment for fistula-in-ano. There are several surgical options, including:
- Fistulotomy: The most common procedure, where the fistula tract is cut open and laid flat to allow it to heal from the inside out. This is often effective for simple fistulas.
- Seton Placement: A seton (a piece of surgical thread) is placed in the fistula tract to help it drain and allow it to heal over time. This technique is often used for complex fistulas or those involving the anal sphincter muscles.
- Advancement Flap Surgery: In cases where the fistula is complex or involves the anal sphincter, an advancement flap surgery may be performed. This involves covering the fistula tract with a piece of healthy tissue from the surrounding area to promote healing.
- LIFT (Ligation of Intersphincteric Fistula Tract): This is a newer technique used for complex fistulas, where the fistula tract is ligated (tied off) to prevent further drainage and encourage healing.
- Fibrin Glue: In certain cases, fibrin glue may be used to seal the fistula tract and promote healing, though this is less common.
(3) Drainage of Abscesses:
If an abscess is present, it must be drained before any surgical treatment of the fistula can take place. This may be done under local anaesthesia or with surgical intervention.
Lifestyle and Supportive Measures
- Proper Hygiene: Keep the anal area clean and dry to reduce the risk of infection. Gentle washing with warm water is recommended after bowel movements.
- High-Fibre Diet: Eating a high-fibre diet helps prevent constipation and reduces the strain during bowel movements, which can aggravate the fistula.
- Hydration: Drinking plenty of water helps keep stools soft and easy to pass, reducing the risk of further irritation to the anal area.
- Avoid Straining: Avoid straining during bowel movements to prevent further injury to the anal region.
Prognosis
With appropriate treatment, most fistulas can be managed successfully. Surgical treatment generally results in significant improvement, and most people are able to recover fully. However, there is a risk of recurrence, especially in people with underlying conditions like Crohn’s disease. Early diagnosis and treatment are essential for preventing complications such as incontinence or chronic infections.
Why Choose Us?
Contact Us