Get Care
Rectal Prolapse
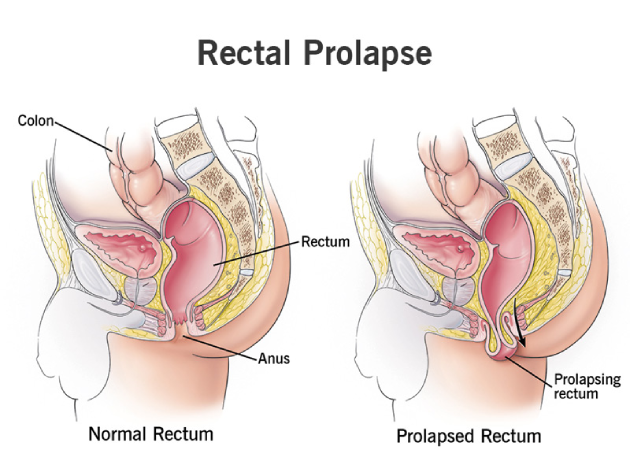
What is Rectal Prolapse?
Rectal prolapse is a condition in which part or all of the rectum (the last portion of the colon) protrudes outside the anus. This occurs when the supporting muscles and tissues that hold the rectum in place become weakened or damaged. Rectal prolapse is more common in older adults, especially women, but it can occur in individuals of any age.The prolapsed portion of the rectum may slide out intermittently, or in severe cases, it may remain outside the body. This condition can range from mild to severe, with symptoms varying depending on the extent of the prolapse.
What Causes Rectal Prolapse?
Several factors contribute to the development of rectal prolapse. These include:
- Weakness of Pelvic Floor Muscles: The muscles and ligaments that support the rectum can become weakened due to aging, childbirth, or chronic straining during bowel movements.
- Chronic Constipation: Long-term constipation and the excessive straining required to pass hard stools can weaken the pelvic floor muscles and lead to rectal prolapse.
- Childbirth: Vaginal delivery, especially multiple deliveries or difficult labor, can stretch and weaken the muscles and tissues supporting the rectum.
- Nerve Damage: Nerve damage, particularly from conditions like spinal cord injuries or neurological disorders (e.g., Parkinson’s disease), can affect bowel control and contribute to rectal prolapse.
- Age: As people age, the connective tissues and muscles naturally lose their strength and elasticity, making older adults more susceptible to rectal prolapse.
- Previous Surgery: Surgery in the pelvic area, particularly involving the colon, anus, or rectum, can contribute to the development of prolapse.
- Genetic Factors: Some individuals may be genetically predisposed to conditions that affect the structure or function of the pelvic floor muscles.
What are the Signs and Symptoms of Rectal Prolapse?
The most common symptoms of rectal prolapse include:
- Protrusion of Rectum: A visible bulge of the rectum outside the anus, which may be more noticeable during bowel movements or when coughing.
- Incontinence: Difficulty controlling bowel movements, leading to fecal incontinence or leakage of stool.
- Sensation of Incomplete Evacuation: Feeling that the bowel has not fully emptied after a bowel movement.
- Pain or Discomfort: A sensation of pressure, pain, or fullness in the rectal area, which may worsen after prolonged sitting or standing.
- Bleeding: Light bleeding from the rectum, often seen on the stool or toilet paper after a bowel movement.
- Mucus Discharge: A mucus discharge from the anus, especially if the prolapsed rectum is exposed to stool or other irritants.
In severe cases, the rectum may remain prolapsed and cannot be pushed back into place manually, leading to persistent discomfort and potential complications.
What are the Risk Factors for Rectal Prolapse?
Certain factors can increase the likelihood of developing rectal prolapse, including:
- Age: Older adults, especially women, are at higher risk due to age-related weakening of muscles and tissues.
- Chronic Constipation: Long-term constipation can lead to straining and increased pressure on the rectum.
- Childbirth: Vaginal childbirth, particularly multiple deliveries or difficult labor, can weaken the pelvic floor and increase the risk of prolapse.
- Neurological Disorders: Conditions that affect nerve function, such as Parkinson’s disease, spinal cord injuries, or multiple sclerosis, can impair bowel control and contribute to prolapse.
- Pelvic Floor Dysfunction: Conditions that weaken or impair the pelvic floor muscles, including prior surgeries or pelvic floor trauma, can increase the risk of rectal prolapse.
- Increased Abdominal Pressure: Obesity or conditions that increase intra-abdominal pressure (e.g., chronic coughing, heavy lifting, or tumors) can contribute to rectal prolapse.
- Genetic Predisposition: A family history of rectal prolapse or related conditions can increase the likelihood of developing the condition.
What are the Complications of Rectal Prolapse?
If left untreated, rectal prolapse can lead to several complications, including:
- Bowel Obstruction: The prolapsed portion of the rectum can become obstructed, preventing the passage of stool and causing severe constipation.
- Fecal Incontinence: Ongoing damage to the rectum and pelvic floor muscles can result in a loss of control over bowel movements.
- Rectal Ulcers: Prolonged exposure of the rectum to the outside environment can lead to the development of sores or ulcers on the prolapsed tissue.
- Chronic Pain: If the rectum remains prolapsed, it can cause persistent pain, discomfort, and difficulty with normal activities.
- Infection: Prolonged exposure of the rectum to bacteria from stool and the external environment can lead to infections or abscess formation
Diagnosis of Rectal Prolapse
Diagnosing rectal prolapse involves a combination of a thorough clinical evaluation, visual inspection, and specialized imaging tests to assess both the presence and severity of the prolapse as well as any contributing disorders.
(1) Medical History and Symptom Assessment
The diagnostic process begins with a detailed medical history. The doctor will ask about:
- Symptoms such as a bulging sensation from the anus, incomplete bowel evacuation, rectal bleeding, mucus discharge, or fecal incontinence
- Duration and progression of symptoms
- Any history of chronic constipation, straining, or pelvic surgery
- Bowel habits, dietary patterns, and urinary symptoms
- Neurological symptoms or history of spinal issues, which may suggest nerve involvement.
Understanding the functional impact on daily life helps determine the urgency and type of treatment needed.
(2) Physical Examination
A rectal exam is usually the first and most important step.
- The patient may be asked to strain or bear down, simulating a bowel movement, which can help the doctor observe the prolapse externally.
- In early or intermittent cases, prolapse may only be visible during straining and not at rest.
- The provider will check for:
- The extent of the prolapse (length and type—partial vs. full thickness)
- Any signs of irritation, ulcers, or infection
- Anal sphincter tone, which is often weakened in long-standing prolapse
- Associated conditions, such as hemorrhoids or mucosal redundancy
(3) Anoscopy
An anoscope (a small, lighted tube) is inserted into the anal canal to inspect:
- The mucosa of the rectum and anal canal
- The origin of the prolapsed tissue, helping differentiate it from hemorrhoids or polyps
- Whether the prolapse involves just the mucosa or the entire rectal wall
This is a quick and minimally uncomfortable procedure, usually done in a clinic setting.
(4) Colonoscopy or Sigmoidoscopy
These tests are used to rule out other gastrointestinal conditions that may mimic or contribute to rectal prolapse, such as:
- Colorectal tumors
- Polyps
- Diverticulosis
- Inflammatory bowel disease
Colonoscopy is typically preferred in older adults or anyone with alarm symptoms like weight loss, bleeding, or family history of colorectal cancer. Sigmoidoscopy may be used when only the distal colon needs to be examined.
(5) Defecography (Evacuation Proctography)
This specialized imaging test is particularly helpful in evaluating functional rectal disorders and internal prolapse that may not be visible externally.
Treatment of Rectal Prolapse
Treatment for rectal prolapse depends on the severity of the condition. In mild cases, conservative management may be sufficient, while more severe cases may require surgical intervention.
(1) Conservative Treatments:
- Dietary Changes: Increasing fiber intake and drinking plenty of fluids to prevent constipation and reduce straining during bowel movements.
- Pelvic Floor Exercises: Strengthening the pelvic floor muscles through exercises (e.g., Kegel exercises) can help improve support for the rectum.
- Bowel Training: Establishing a regular bowel routine and avoiding straining can help manage symptoms.
(2) Surgical Treatment:
- Rectopexy: A surgical procedure in which the prolapsed rectum is repositioned and secured to the sacrum (a bone in the lower back) to prevent future prolapse.
- Resection of Prolapsed Rectum: In severe cases, a portion of the prolapsed rectum may need to be surgically removed.
- Perineal Proctectomy: This procedure involves removing the rectum through the perineum (the area between the anus and the genitals) and is typically reserved for older patients or those who are not candidates for abdominal surgery.
- Stapled Rectal Surgery: A minimally invasive surgery that uses staples to remove excess tissue and secure the rectum in place.
(3) Postoperative Care:
After surgery, patients are typically advised to follow a high-fiber diet, use stool softeners to avoid constipation, and perform pelvic floor exercises to maintain muscle strength.
Lifestyle and Supportive Measures
To prevent or manage rectal prolapse, individuals should adopt the following habits:
- Avoid Straining: Practice healthy bowel habits to avoid excessive straining during bowel movements.
- Maintain a Healthy Weight: Reducing abdominal pressure by maintaining a healthy weight can help prevent rectal prolapse.
- Regular Exercise: Engaging in regular physical activity, including pelvic floor exercises, can help strengthen the muscles that support the rectum.
- Eat a High-Fiber Diet: A fiber-rich diet can prevent constipation and reduce the need for straining.
- Seek Early Medical Attention: If you experience symptoms like a prolapsed rectum or fecal incontinence, seeking medical advice early can help prevent further complications.
Prognosis
The prognosis for individuals with rectal prolapse depends on the severity of the condition and the treatment approach. Most cases can be successfully managed with conservative treatments or surgery. However, if left untreated, rectal prolapse can lead to significant complications, including chronic pain, bowel obstruction, and incontinence.
Why Choose Us?
Contact Us