Get Care
Ventral Hernia
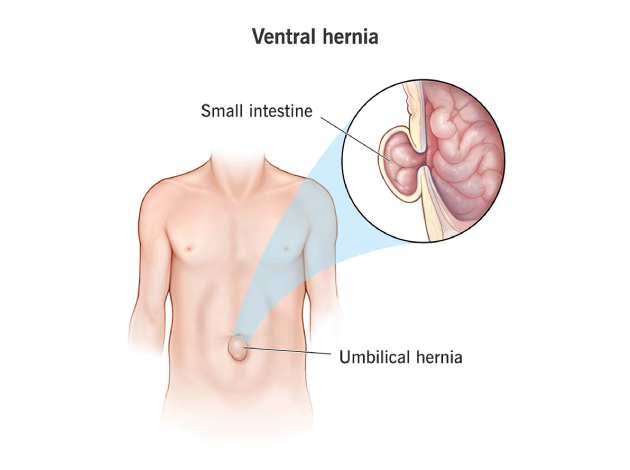
What is a Ventral Hernia?
A ventral hernia is a bulge of tissues through an opening or weakness in the abdominal wall muscles. It typically occurs in the midline (front) of the abdomen and can develop at natural weak points, post-surgical incision sites, or due to acquired weakening of the abdominal muscles. Unlike groin hernias (inguinal or femoral), ventral hernias are located in the anterior (front) abdominal wall and include umbilical, epigastric, and incisional hernias.Ventral hernias may remain small and asymptomatic for a long time but can enlarge over time, causing discomfort, pain, and risk of complications like incarceration or strangulation of intestines.
What Causes a Ventral Hernia?
A ventral hernia occurs when a weakness in the abdominal wall allows tissue or organs to bulge outward. It can result from increased abdominal pressure or weakened muscles. Common causes include:
- Previous abdominal surgery, especially with poor healing, leading to incisional hernias
- Congenital weakness in the abdominal wall (e.g., umbilical hernias)
- Obesity, which adds strain on the abdominal muscles
- Chronic coughing or straining from respiratory issues or constipation
- Heavy lifting without proper technique
- Pregnancy, which stretches and weakens abdominal muscles
- Ascites (fluid buildup in the abdomen)
- Infection or poor wound healing after surgery
Symptoms of Ventral Hernia
Symptoms depend on the size and contents of the hernia and may include:
- Visible bulge or swelling on the abdominal wall – More noticeable when standing or straining
- Dull ache or discomfort at the hernia site
- Pain worsened by lifting, coughing, or prolonged standing
- Feeling of heaviness or pressure in the abdomen
- Difficulty bending or performing physical activity
- Redness, tenderness, or sudden pain at the site (suggesting strangulation)
In some cases, hernias may become incarcerated (non-reducible) or strangulated (blood supply to contents is cut off), which is a surgical emergency.
What are the Risk Factors for a Ventral Hernia?
Previous Abdominal Surgery – Incisions weaken the abdominal wall, leading to incisional hernias.
Obesity – Excess weight increases pressure on the abdominal muscles and delays healing.
Advanced Age – Aging reduces muscle strength and healing capacity.
Smoking – Impairs tissue healing and causes chronic coughing, which strains the abdominal wall.
Diabetes Mellitus – Slows wound healing and raises infection risk.
Poor Nutrition – Deficiencies in protein and key vitamins weaken tissue and delay healing.
Heavy Physical Work – Frequent lifting or straining raises intra-abdominal pressure.
Chronic Cough or Constipation – Both increase abdominal pressure and strain the abdominal wall.
What are the Complications of a Ventral Hernia?
If untreated or improperly managed, ventral hernias can result in:
- Incarceration – Herniated contents become trapped and cannot be pushed back
- Strangulation – Blood supply to herniated tissue is compromised, leading to tissue death
- Bowel obstruction – Due to kinking or entrapment of intestines
- Chronic pain and discomfort
- Skin changes or ulceration over the hernia site
- Recurrence after surgical repair, especially without mesh
Diagnosis of Ventral Hernia
The diagnosis of a ventral hernia is primarily clinical, based on history and physical examination. However, imaging modalities are often used in cases where the diagnosis is uncertain or when detailed anatomical information is required for surgical planning.
(1) Physical Examination
The hallmark sign of a ventral hernia is a visible or palpable bulge on the abdominal wall. Important characteristics include:
- Bulge Appearance: The bulge typically becomes more prominent with straining, coughing, or standing, and may reduce (disappear) when the patient lies down.
- Reducibility: Many hernias are reducible, meaning the contents of the hernia sac can be pushed back into the abdominal cavity manually or by gravity.
- Tenderness or Pain: A tender or irreducible hernia may suggest complications such as incarceration (trapped contents) or strangulation (compromised blood supply).
- Incisional History: For incisional hernias, the examination often reveals a bulge near or along a previous surgical scar.
(2) Ultrasound of the Abdomen
Ultrasound is a non-invasive, widely available imaging modality useful for:
- Detecting small, occult, or intermittent hernias that are not obvious on physical exam.
- Evaluating contents of the hernia sac (fat, bowel loops, etc.).
- Useful in pediatric, thin, or pregnant patients, where radiation exposure from CT should be avoided.
(3) CT Scan (Computed Tomography)
A CT scan of the abdomen and pelvis is the most accurate and commonly used imaging method for ventral hernia assessment, especially in pre-operative planning:
- Provides a comprehensive view of the hernia’s size, contents, and location.
- Identifies multiple hernia defects, strangulation, or bowel obstruction.
- Helps differentiate hernias from other abdominal wall or intra-abdominal masses.
- Essential in cases of recurrent hernias or when surgery is being considered.
(4) MRI (Magnetic Resonance Imaging)
MRI is rarely used, but may be indicated in:
- Complex, recurrent, or post-surgical cases where tissue planes are difficult to distinguish.
- Patients who cannot undergo CT scans (e.g., due to contrast allergies or renal impairment).
- MRI offers excellent soft tissue contrast, making it useful in identifying mesh complications or soft tissue involvement.
Treatment of Ventral Hernia
The treatment of a ventral hernia depends on the severity of symptoms, size of the hernia, risk of complications, and the patient’s overall health. While surgical repair is the definitive treatment, non-surgical (conservative) approaches may be used in select cases. The medical management for ventral hernia includes:
(1) Pain Management
Analgesics (e.g., acetaminophen, NSAIDs)
To relieve mild to moderate abdominal discomfort.Avoid narcotics long-term as they can cause constipation and worsen symptoms.
(2) Management of Associated Symptoms
Laxatives or stool softeners (e.g., lactulose, docusate sodium):
Used to prevent straining during bowel movements.Antacids or PPIs (e.g., omeprazole, pantoprazole):
If GERD-like symptoms are present due to abdominal pressure.Antibiotics:
Only used if infection is suspected—e.g., in case of a strangulated or incarcerated hernia with signs of sepsis.
(3) Supportive Devices
Abdominal binders or hernia trusses:
Offer temporary support and reduce bulging, especially in high-risk or non-surgical patients.
(4) Monitoring and Risk Management
Weight loss programs: To reduce intra-abdominal pressure.
Smoking cessation: To promote better healing and reduce chronic cough.
Treatment of chronic cough or constipation: Minimizes strain on the hernia.
Why Choose Us?
Contact Us